
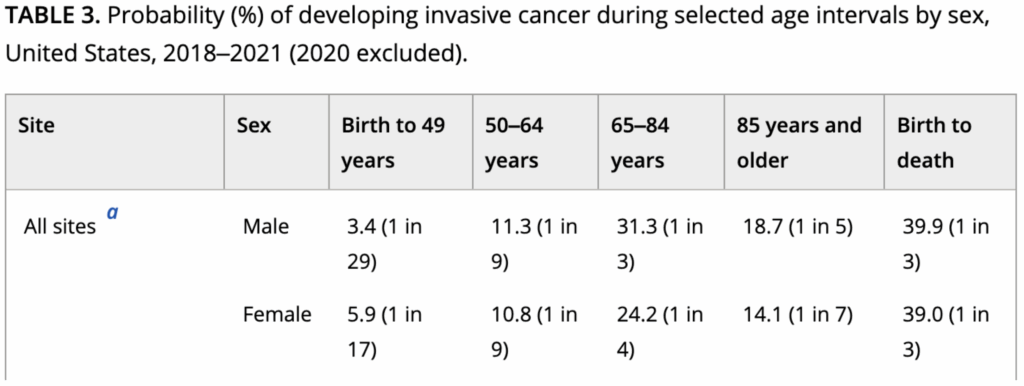
You will be affected by cancer in your lifetime. Whether that be directly or via a loved one, only time will tell. According to recent study released in 2025, 39.9% of men and 39.0% of females will develop an invasive cancer during their lifetime.1 See table below for age related breakdown from this study.
In a miraculously beautiful yet ever increasingly toxic world (environmental, psychological, sociopolitical), cancer is poised to become ever more prevalent. Based upon our current trajectory regarding the Standard American Diet (SAD), chronic stress resulting from neurological overstimulation and sympathetic branch of autonomic nervous system hyperarousal, propensity to overwork, lack of time allocated for restoration and rejuvenation, sleep deprivation combined with circadian dysregulation, unrealistic expectations regarding what we should be doing/accomplishing, an epidemic of social isolation coated in a veneer finish of social media, along with an ever increasing global toxic burden exposure load, and there is no possible way that cancer incidence rates will drop or even sustain the status quo without a fundamental shift in our collective consciousness and ways of living.
As a Functional, Integrative, Family, and Environmental Medicine boarded/certified physician, I recognize the problem. It is not the cancer that is the disease. Our current state of existence within our not so natural environment and the perpetual existential crises that arises from this misalignment is a if not the root cause. Cancer, like autoimmune dysregulation, cardiometabolic diseases, and other chronic medical conditions are simply the symptoms of a deeper and more insidious issue, i.e. how we live. The current state of affairs is considered “normal” via our collective social programming and seamlessly grooved within our socially conditioned and reinforced neurological software. Although this may come be surprising, studies reveal that Only 5–10% of all cancer cases can be attributed to genetic defects (i.e. BRCA mutations and breast cancer, Lynch Syndrome), whereas the remaining 90–95% have their roots in the environment and lifestyle. The lifestyle factors include cigarette smoking, diet (fried foods, red meat), alcohol, sun exposure, environmental pollutants, infections, stress, obesity, and physical inactivity.2
Upon closer inspection, it becomes readily apparent that a paradigm shift in consciousness is necessary to deliver us from the current state of a disease-oriented society to one of salutogenesis, which is an approach to health and well-being that focuses on the origins and maintenance of health, rather than the causes of disease.3 In that same vein, why would we continue providing a one size fits all approach to cancer therapy when every single individual is fundamentally different in their genetic predispositions, environmental exposures, risk factors for their specific tumor, lifestyle habits, and belief systems? It truly defies logic, especially when one takes into consideration that even within a specific subset of cancer patients (women in their 40s-50s with Stage III or IV Intraductal Carcinoma that is ER+/PR+/HER2 negative/Ki67>50%), these patients will have a bell curve distribution of clinical responsiveness to a premeditated therapeutic intervention.
Might it be more logical, clinically effective, and humane to provide an individualized therapy protocol based upon a person’s specific tumor chemosensitivities (i.e. testing specific chemotherapies and natural agents on the person’s circulating tumor cells to determine the most effective therapies)? The answer is so obvious that it is rhetorical in nature. This technology actually exists and is available to anyone with cancer. See RGCC Onconomics Plus Report Summary below:
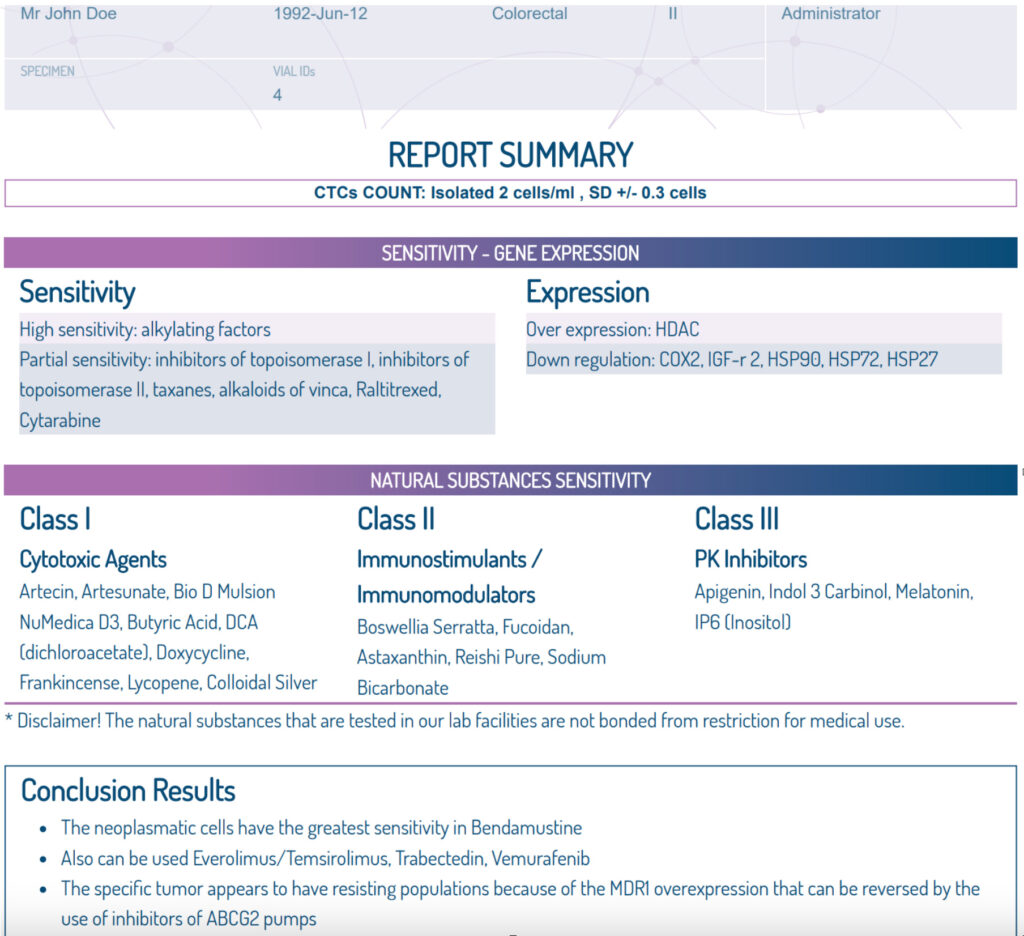

On September 13, 2025, I gave a presentation at the RGCC Gathering International Conference in Zurich, Switzerland regarding this advanced and personalized cancer testing. It was inspiring to see more and more Oncologists and other Integrative Oncology providers utilizing this life changing technology to improve the health outcomes for their patients. Several recent studies validate the effectiveness of choosing chemotherapeutic agents with higher cytotoxicity effectiveness based upon that patient’s specific RGCC Onconomics Plus testing. One study of patients with metastatic colorectal cancer had a survival duration of 9 months vs the 5.15 month survival duration within the control group.4 Another study utilizing the Onconomics Plus testing on circulating tumor cells for choosing second line chemotherapy agents in pancreatic cancer revealed a medium survival for the Onconomics Plus treatment group of 7 months which was significantly greater than the median survival duration of the two best supportive care groups, which was 2.29 and 2.4 months, respectively.5 Beyond these early clinical trials, I functionally utilize this advanced and personalized cancer testing in my clinic by helping patients choose natural cytotoxic agents (i.e. Vit D, Vit C, Melatonin, Curcumin, etc.) and off label medications (i.e. Low Dose Naltrexone, Ivermectin, Doxycycline) that have demonstrated effectiveness as cytotoxic agents for that particular patient’s circulating tumor cells (CTCs). We also track their CTC count every 4 – 6 months to determine therapy responsiveness. Perhaps even more beneficial is that I can now share objective evidence where the patient’s prescribed chemotherapy and/or hormone blocking medication (in ER+ breast cancer and prostate cancer) may be effective. This approach to collaborating with the patient’s oncology team (Oncologist, Surgical Oncologist, Radiation Oncologist) has been radically successful in helping the patient to utilize the best of both worlds versus a more polarizing either/or philosophy. For more insight into the unification of Integrative Oncology with the standard of care cancer therapies, please see my article: “Cancer, the Unnecessary Tragedy”.
I look forward to the day when this is simply standard of care therapy. Until that time, please reach out to me at www.metamedical.life or another RGCC Accredited Practitioner. I sincerely hope that you find this both inspiring and empowering. Wishing you and your loved ones the best in your healing and wellness journey towards optimal vitality and ultimately living your most authentic and embodied life.
Manifest your METAmorphosis,
Clayton Bell, M.D.
META Medical PLLC
Citations
1. Siegel RL, Kratzer TB, Giaquinto AN, Sung H, Jemal A. Cancer statistics, 2025. CA Cancer J Clin. 2025 Jan-Feb;75(1):10-45. doi: 10.3322/caac.21871. Epub 2025 Jan 16. PMID: 39817679; PMCID: PMC11745215.
2. Anand P, Kunnumakkara AB, Sundaram C, Harikumar KB, Tharakan ST, Lai OS, Sung B, Aggarwal BB. Cancer is a preventable disease that requires major lifestyle changes. Pharm Res. 2008 Sep;25(9):2097-116. doi: 10.1007/s11095-008-9661-9. Epub 2008 Jul 15. Erratum in: Pharm Res. 2008 Sep;25(9):2200. Kunnumakara, Ajaikumar B [corrected to Kunnumakkara, Ajaikumar B]. PMID: 18626751; PMCID: PMC2515569.
3. Mittelmark MB, Bauer GF. Salutogenesis as a Theory, as an Orientation and as the Sense of Coherence. 2022 Jan 1. In: Mittelmark MB, Bauer GF, Vaandrager L, et al., editors. The Handbook of Salutogenesis [Internet]. 2nd edition. Cham (CH): Springer; 2022. Chapter 3. Available from: https://www.ncbi.nlm.nih.gov/books/NBK584092/ doi: 10.1007/978-3-030-79515-3_3
4. Drevs J, Malhotra MS, Sahinbas H, Iliopoulos A, Beis G, Apostolou P, Papasotiriou I. Adjusting Treatment Strategies Using Circulating Tumor Cells: Preliminary Results on Metastatic Colorectal Cancer. Anticancer Res. 2025 Feb;45(2):491-502. doi: 10.21873/anticanres.17438. PMID: 39890201.
5. Drevs J, Malhotra MS, Sahinbas H, Iliopoulos A, Beis G, Apostolou P, Papasotiriou I. Second-line therapy adjustment for advanced pancreatic cancer using circulating tumor cells: Preliminary results. Cancer Treat Res Commun. 2025;44:100956. doi: 10.1016/j.ctarc.2025.100956. Epub 2025 Jun 20. PMID: 40554947.